Cataract Surgery - Vitreous Opacities & Retroillumination Techniques
Cataract surgery in the presence of vitreous opacities, such as in vitreous hemorrhage or endophthalmitis, is often combined with pars plana vitrectomy. Even so, the cataract surgery is often very challenging due to the absence of the red reflex.
While vitreous opacities in some patients can be a mere nuisance, in others they can be visually significant and interfere with daily activities.
The traditional teaching has been to simply educate patients that vitreous floaters are a benign condition with no long-term sequelae and observe them.
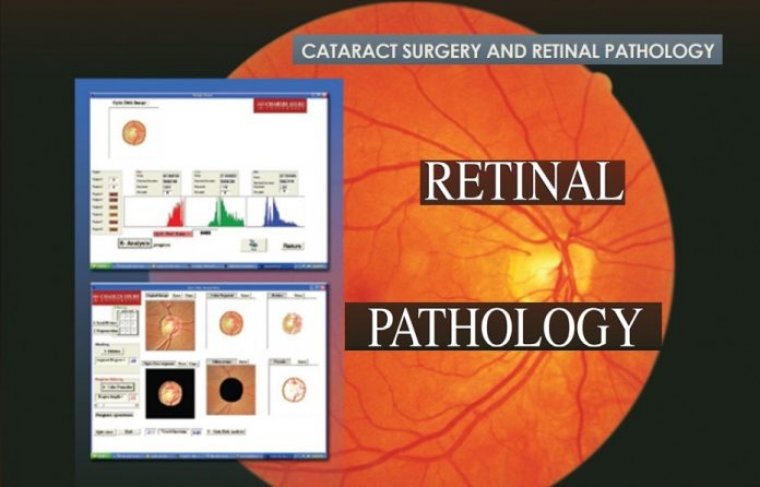
Multimodal imaging is a helpful tool for the clinical assessment of VOs. Several imaging tests can aid in our evaluation of the vitreous and help to educate the patient about how their symptoms correlate with their anatomical findings.
The first test is scanning laser ophthalmoscopy imaging on optical coherence tomography to assess the shadowing of the vitreous.
On the main OCT image, the hyaloid face separation from (or adherence to) the retina can be visualized.
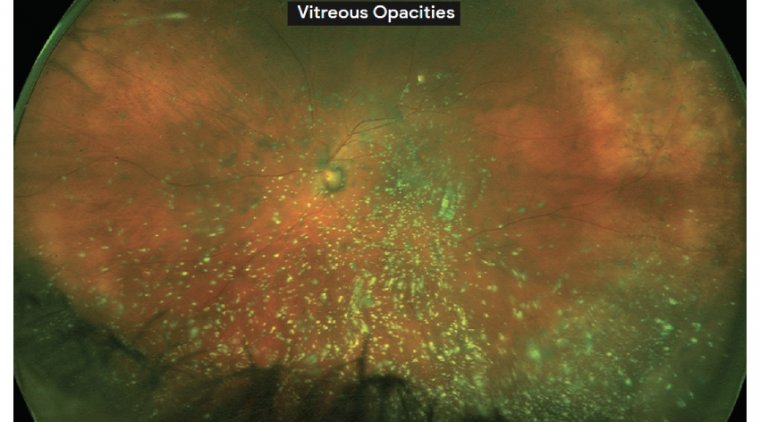
Widefield fundus photography and autofluorescence can help about the anatomy of the vitreous and retina, and to highlight any peripheral pathology.
Although it’s not used routinely in clinical practice, ultrasound can also be helpful to quantify vitreous opacities and correlate them with disease severity.
Cataract surgery can be difficult to perform when dense vitreous opacities are present, due to the absence of the red reflex.
Even when cataract surgery is combined with vitrectomy, this difficulty still exists because, in many cases, the view is too poor to permit vitrectomy to clear the vitreous opacities before removal of the cataract.
Dr Joseph W. Fong and Dr Ahmed A. Sallam, both from the Harvey & Bernice Jones Eye Institute at the University of Arkansas for Medical Sciences in Little Rock, Arkansas, United States, shared their pearls for improving the visualisation in these eyes using retroillumination techniques that include a 25-gauge chandelier or a light pipe.
Retroillumination configurations using the chandelier - The doctors described two configurations using the 25-gauge chandelier.
In the first, the chandelier was directed down towards the vitreous. In the case being demonstrated, the patient had a dense vitreous haemorrhage due to diabetic retinopathy.
Dr Fong advised that the view can often be improved in this scenario by extinguishing the room and microscope lights and by depending only on the retroillumination provided by the chandelier.
In a second case, Drs Fong and Sallam demonstrated the view achieved when the chandelier was directed horizontally or towards the lens.
“Directly illuminating the lens from behind provides the surgeon with crisp and detailed visualisation of the lens structure and is often very helpful in cases where vitreous haemorrhage is very dense,” Dr Fong said.
Retroillumination via light pipe - In another case of a patient with a dense vitreous haemorrhage from diabetic retinopathy, Dr Fong showed how to maximise use of the light pipe.
As in the previous case using the chandelier, maximum visualisation was achieved when the lights from the microscope and rooms were turned off .
Dr Fong explained that a light pipe has an advantage compared with a chandelier because an experienced vitreoretinal surgeon has real-time control over the position of the light pipe at all times intraoperatively.
However, use of the light pipe means that the surgeon has to perform the procedure using one hand, which is a major disadvantage. The surgeon does have the option of removing the light pipe to chop the nucleus using both hands.
After the chop procedure is completed, the light pipe can be re-inserted to facilitate a better view of the cortex to be removed. “The chandelier and light pipe are both great options to achieve retroillumination and optimal visualisation during these challenging cataract surgeries,” Dr Fong said.
“Using the chandelier has an advantage over the light pipe in that the surgeon can use both hands throughout cataract surgery. This frees the surgeon from concerns about the position of the light source and facilitates his or her concentration on the details of the challenging surgery.”
Another challenging surgical scenario is encountered in cases of active endophthalmitis. Dr Fong demonstrated insertion of a light pipe into a trocar to retroilluminate the lens during the capsulorhexis.
The light pipe was then inserted through the limbal side port to illuminate the lens during phacoemulsifi cation. “These retroillumination techniques can be used to conquer cataract surgery when many diff erent types of vitreous opacities are present,” Dr Fong concluded.
Let's Check What Others Think & Say